
Medical coding systems are standardized code sets and classification systems that translate clinical encounters into alphanumeric codes. ICD-10-CM and ICD-10-PCS capture diagnoses and inpatient procedures, CPT describes services, and HCPCS Level II covers supplies and transport — together they document, analyze, and bill medical services consistently.
For healthcare providers, medical coding sits at the center of medical billing and reimbursement. It’s also complex. As you set up workflows, it’s normal to ask, “What are ICD-10 codes?” or “How do I choose the right code for this visit?” Clear, consistent coding helps reduce claim denials, shortens payment cycles with payers, and ultimately supports better patient care.
This guide explains the major medical coding systems used across the healthcare industry. You’ll see how ICD-10-CM and ICD-10-PCS record diagnoses and inpatient procedures, how CPT details services, and how HCPCS Level II covers supplies and equipment.
We will provide practical examples, point to trustworthy sources, and show how a firm grasp of these code sets improves clinical documentation and daily operations.
Medical coding systems at a glance
Understanding the main code sets helps you choose the right classification systems for each encounter and ensure accurate billing. Here’s how the core systems work together across healthcare settings.
- ICD-10-CM (diagnoses): Records conditions, symptoms, and reasons for visits across outpatient and inpatient care. It improves documentation, analytics, and reporting.
- ICD-10-PCS (inpatient procedures): Describes hospital procedures for stays that require admission. It supports grouping for payment and clinical analysis.
- CPT (services): Details medical procedures and diagnostic services performed by clinicians in outpatient care. Categories I, II, and III cover established services, performance tracking, and emerging tech.
HCPCS Level II (supplies and transport): Reports items not in CPT, such as durable medical equipment, orthotics, and ambulance services, so claims reflect everything delivered. - DRG (payment grouping): Groups inpatient cases with similar clinical traits and expected resource use. It ties coded data to hospital payment and audit review.
Together, these systems create a complete record for clinicians, coders, and payers, reducing ambiguity and supporting accurate reimbursement.


"Understanding the main code sets helps you choose the right classification systems for each encounter and ensure accurate billing."
ICD-10 overview (history, governance, cadence)
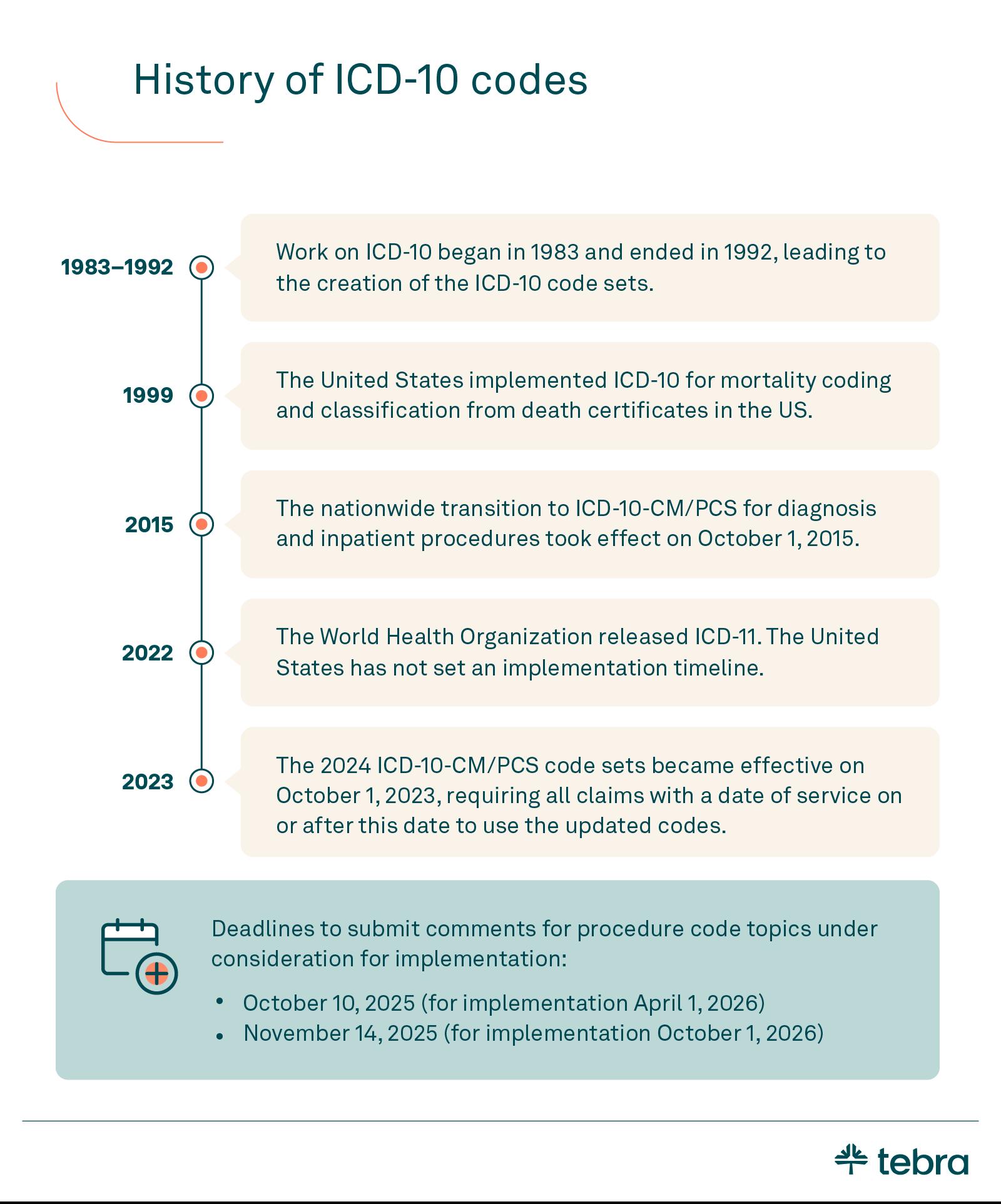
The International Classification of Diseases began its tenth revision in 1983 to reflect advances in medicine and data needs. The United States adopted ICD-10 for mortality reporting in 1999, then completed the nationwide transition to ICD-10 codes for diagnosis and inpatient procedures on October 1, 2015. The World Health Organization owns the core ICD standard, while US health agencies adapt and maintain it for care and billing.
In the US, the NCHS/CDC oversees the clinical modification of ICD-10 for diagnoses. See the CDC’s page on ICD-10-CM for current materials and guidance. The Centers for Medicare & Medicaid Services manage ICD-10-PCS for inpatient procedures, including specification files and update schedules.
CMS publishes procedure updates and technical files on its site. For continuity, we will reference the same CMS destination used in your original draft.
Update cadence matters in daily coding. ICD-10-CM typically updates annually for the fiscal year that starts on October 1. ICD-10-PCS updates occur on a biannual cycle aligned with inpatient payment and reporting needs. Each cycle may introduce new codes, deletions, and clarifications through the ICD-10 Coordination and Maintenance Committee, with public materials and meeting notes made available for review.
The ICD-11, released by WHO, is gaining traction globally. The US has not set an implementation date, so practices should continue to follow ICD-10-CM and ICD-10-PCS. For historical update lists, WHO maintains an archive of official ICD-10 updates on its site. See the WHO ICD-10 updates page for context.
ICD-10-CM structure and use
The ICD-10-CM clinical modification uses alphanumeric codes that are 3 to 7 characters. The first character is a letter. Characters 2 and 3 are numbers. Characters 4 through 7 add clinical detail. A placeholder “X” fills unused positions when needed.
Codes capture laterality, episode of care, severity, and complications, allowing clinicians to select appropriate codes and correct codes with less ambiguity.
The scope is broad. Chapters span A00 — Z99 for diseases, signs, and external causes, with U00 — U85 reserved for special purposes. You can browse the official ICD-10-CM browser on the CDC website for current lists, guidelines, and addenda, and check the CDC’s maintenance page for timing and technical notes from ICD-10-CM resources.
"The ICD-10-CM clinical modification uses alphanumeric codes that are 3 to 7 characters."
Structure supports the maintenance of clean patient records and the exchange of reliable health information in daily work. Accurate selection drives problem lists, orders, and referrals in the outpatient setting, helping to align documentation with payer policies.
Clear coding improves charge capture and reduces audit risk by matching notes to codes and official coding guidelines. It also enables quality reporting and timely follow-up because conditions are recorded consistently across encounters.
Tie coding to your clinical workflow inside the EHR. Templates, favorites, and decision support can surface likely codes while you chart. A system like Tebra’s EHR software lets teams search the catalog, apply edits, and keep files current, ensuring workflows remain efficient from charting to claims.
When rules change, updates automatically reflect in the picker. That reduces rework, shortens denials, and supports internal audits before the claim leaves your practice.
Who uses ICD-10-CM?
Healthcare providers use ICD-10-CM to document conditions in patient records and support orders, referrals, and follow-up.
Here is who relies on ICD-10-CM across care and billing workflows:
- Healthcare providers: Use it to document conditions in patient records and support orders, referrals, and follow-up.
- Medical coders: Translate notes into appropriate codes and correct codes for the billing process and internal audits.
- Hospitals and clinics: Apply it for quality reporting, utilization reviews, and consistent health information across encounters.
- Insurance companies and other payers: Check medical necessity and adjudicate reimbursement.
- Public health agencies: Analyze trends and monitor outbreaks to inform public health action.
- Researchers and academic programs: Study outcomes and train coding professionals using standardized data.
ICD-10-CM codes are used by providers, coders, hospitals, insurers, public health agencies, and researchers to document conditions, support billing, monitor outcomes, and improve patient care.
With EHR workflows embedded, consistent use of ICD-10-PCS enhances accuracy across both outpatient and inpatient settings, aligning with official coding guidelines.
ICD-10-PCS vs. ICD-10-CM
ICD-10-PCS is the hospital procedure coding system used for inpatient stays. It specifies how a procedure was performed, including approach, device, and body part, and it drives grouping and payment logic. CMS posts the official specifications and yearly files on its ICD-10-PCS updates page.
ICD-10-CM captures diagnoses across all settings. It records conditions, symptoms, and reasons for visits, which establish medical necessity for diagnostic services and treatment plans. The CDC maintains the current code lists and guidelines in its ICD-10-CM resources.
When used together, the CM explains why the patient needed care, and the PCS explains what the hospital did. The pairing supports accurate DRG assignment, tighter documentation, and fewer edits during the billing process.
ICD-9 vs. ICD-10 – Why the shift?
The transition from ICD-9 to ICD-10 codes occurred because the older system had reached its capacity and could no longer describe modern medicine with sufficient specificity. Health systems require clearer diagnoses, laterality, and better data for quality and payment.

The change is documented in the NCHS ICD resources and outlined in the ICD-10-CM FAQ from the CDC, with historical context in this ICD-9 overview from NCBI.
- Structure: ICD-9 used 3 to 5 mostly numeric characters. ICD-10 uses 3 to 7 alphanumeric characters with placeholders and extensions, which helps coding professionals capture details and choose the correct codes.
- Specificity and laterality: ICD-10 adds severity, encounter timing, and left vs. right, which improves clinical accuracy and downstream analytics compared with ICD-9.
- Coverage and usability: ICD-10 dramatically expands the code set, accommodates new therapies and technologies, and supports more precise documentation that aligns notes with claims.
The result is cleaner charts, fewer mismatches at adjudication, and a coding language that better reflects contemporary care.
Social determinants of health (Z codes)
Social determinants of health appear in ICD-10-CM as Z codes, which provide context about nonclinical health conditions that influence patient care. These entries help clinicians document factors that shape outcomes and enable planners to design public health programs.
Z codes account for less than 1% of the roughly 70,000 diagnosis codes, yet they support practical initiatives in analytics and care coordination. You can review the official structure and guidelines in the CDC’s ICD-10-CM resources and the ICD-10-CM browser.
Common SDOH Z code categories:
- Z55: Problems related to education and literacy
- Z56: Problems related to employment and unemployment
- Z59: Problems related to housing and economic circumstances
- Z60: Problems related to the social environment
- Z62: Problems related to upbringing
- Z63: Other problems related to the primary support group, including family circumstances
- Z65: Problems related to other psychosocial circumstances
Used consistently, these codes enrich patient care plans, inform referrals, and support population reporting. For current lists and notes, see the CDC’s ICD-10-CM resources and the live ICD-10-CM browser.
"Used consistently, these codes enrich patient care plans, inform referrals, and support population reporting."
CPT and HCPCS (Level I and Level II)
Current Procedural Terminology (CPT) is the Level I portion of the Healthcare Common Procedure Coding System. Maintained by the AMA, CPT codes describe clinician-performed services and diagnostic services across outpatient care, including radiology, pathology, surgery, and medicine. CPT has 3 categories that work together:
- Category I: Routine, widely used services with FDA clearance where applicable. Structured in sections like evaluation and management, anesthesia, surgery, radiology, pathology, laboratory, and medicine.
- Category II: Performance-measurement codes, reported in addition to a service to track quality, and they are optional and not paid separately.
- Category III: Temporary codes for emerging technology, services, and procedures are used for data collection until they graduate to Category I or are sunset.

The AMA publishes the code set and periodic updates. These PLA (proprietary laboratory analyses) additions are issued quarterly within the CPT ecosystem. You can review the official structure in the AMA’s CPT code sets.
Accurate use often depends on modifiers. These two-character appendices explain circumstances that change a service without altering the base code, such as bilateral procedures, discontinued services, or professional versus technical components in radiology. Clean modifier use helps reflect clinical reality, supports medical necessity, and reduces rework in claims.
"Accurate use often depends on modifiers."
HCPCS codes Level II, maintained by CMS, complement CPT by representing supplies, drugs, ambulance transport, and equipment not captured in CPT — think durable medical equipment, prosthetics, orthotics, and certain drugs and biologics. Level II codes are alphanumeric and updated on a set annual cycle.
The CMS posts current files, ground rules, and application pathways on its HCPCS Level II pages.
A note on naming: HCPCS historically referenced “Level III” local codes, which some payers and state agencies use. CMS discontinued those local codes after national standardization efforts, so in practice, HCPCS now functions with Level I (CPT) and Level II only.
Used together, CPT and HCPCS Level II provide clinicians and coders with a comprehensive vocabulary for services, as well as supplies, ensuring clear documentation and accurate claims across various settings.
DRG and payer context (Medicare + MACs)
Hospital reimbursement in the US relies on diagnostic-related group assignment. Medicare’s inpatient prospective payment system pays inpatient claims and groups encounters by diagnosis and resource use.
Accurate diagnoses from ICD-10-CM and procedures from ICD-10-PCS flow into the grouper, so documentation quality directly affects payment and audit exposure during the billing process.
The Centers for Medicare & Medicaid Services administers Medicare, but regional Medicare Administrative Contractors handle day-to-day operations. MACs enroll providers, process claims, educate practices, and publish local coverage guidance that influences reimbursement decisions. You can confirm policies and coding requirements for specific services in CMS’s Medicare Coverage Database.
Private payers and insurance companies often follow similar logic, using diagnosis and procedure data to evaluate medical necessity and price claims. When codes, notes, and orders tell the same clinical story, adjudication is faster and denials drop.
The practical takeaway is simple. Use precise diagnosis codes to explain why the patient required care, pair them with the correct inpatient procedures upon admission, and keep supporting documentation tight so grouping and pricing are accurate the first time.
"When codes, notes, and orders tell the same clinical story, adjudication is faster and denials drop. "
How to look up codes (step by step)
Use this quick workflow to select appropriate codes and correct codes, then reflect them in your EHR.
- Diagnoses in ICD-10-CM: Open the CDC’s ICD-10-CM browser. Search by term or code. Read inclusions, exclusions, and “use additional” notes. Copy the code and paste it into your medical records template.
- Inpatient procedures in ICD-10-PCS: Download the CMS ICD-10-PCS updates. Confirm body system, root operation, approach, device, and qualifier using the tables and index.
- Services in CPT: Check the AMA CPT code sets. Pick the service, then verify section guidelines and parenthetical instructions. If it is a lab assay, review CPT PLA codes for quarterly additions.
- Supplies and transport in HCPCS Level II: Use CMS HCPCS Level II to confirm descriptors, units, and quarterly changes.
- Coverage and policy check: Search CMS’s Medicare Coverage Database for LCDs and NCDs that affect the claim.
- EHR application: Add the selection to Tebra’s EHR software so the code flows to orders and ePrescribing (eRx) without retyping.
Submitting requests for new or revised codes (MEARIS + CDC/NCHS)
For inpatient procedures, the Centers for Medicare & Medicaid Services accepts proposals for new codes and deletions through MEARIS. Use the public MEARIS portal to submit background materials and track status for ICD-10-PCS requests, then follow CMS’s published process for requesting new or revised ICD-10-PCS procedure codes.
Diagnoses follow a separate path. For ICD-10-CM, submit proposals to NCHS/CDC using the templates on the CDC’s ICD-10-CM maintenance page. Include clinical rationale, proposed titles, and where the change belongs in the hierarchy.
Both agencies review proposals at the public ICD-10 Coordination and Maintenance meetings. Sessions are streamed as a webinar, and meeting materials outline decisions and next steps.
When adopted, updates are posted in the annual addenda and typically take effect on October 1. Plan your internal timelines to test initiatives that depend on new or revised codes in your EHR and billing tools before they go live.
"When adopted, updates are posted in the annual addenda and typically take effect on October 1."
Common, unusual, and 2024 examples
Choosing proper codes for everyday visits and accurately coding procedures helps medical coders prevent claim denials and expedite payment. Here are the examples from the original article, retained and grouped by setting. Use these as quick references when documenting diagnostic services and routine care.
Family medicine
Primary care
Mental health
Orthopedics
- M19.041: Primary osteoarthritis, right hand
- M19.241: Secondary osteoarthritis, right hand
- M05.432: Rheumatoid myopathy with rheumatoid arthritis of the left wrist
- M54.50: Low back pain, unspecified
Urgent care
- J02.8: Acute pharyngitis due to other specified organisms
- J06.9: Acute upper respiratory infection, unspecified
- R07.1: Chest pain on breathing
- Z00.00: Encounter for general adult medical exam without abnormal findings
- Z00.129: Encounter for routine child health examination without abnormal findings
Unusual codes
Most ICD-10 codes describe common medical conditions and procedures. However, some codes capture unusual or rare situations:
- V97.33XD: Sucked into a jet engine, subsequent encounter
- W56.22XA: Struck by orca, initial encounter
- Z63.1: Problems in relationships with in-laws
- V91.07XA: Burn due to water skis on fire, initial encounter
- W61.12XA: Struck by macaw, initial encounter
- Y93.D1: Activity, knitting and crocheting
- V95.41XA: Spacecraft crash injuring occupant, initial encounter
- Y92.253: Opera house as the place of occurrence of the external cause
- W220.2XD: Walked into a lamppost, subsequent encounter
Examples of new codes in 2024/25
In 2024, CMS introduced 526 new billing codes. The new codes include the following:
- W44.B3xA: Plastic toy and toy part entering into or through a natural orifice, initial encounter
- Z62.23: Child in custody of a non-parental relative
- Z62.823: Parent-step child conflict
- M80.8B2P: Other osteoporosis with current pathological fracture, left pelvis, subsequent encounter for fracture with malunion
- H50.662: Superior oblique muscle entrapment, left eye
How core medical coding systems compare across use cases
A quick side-by-side helps teams see how the major classification systems and code sets fit together for clinicians, providers, and payers. Use this as a reference when selecting codes for documentation and reimbursement.
| Comparison: Core Medical Coding Systems | ||||
|---|---|---|---|---|
| Coding system | Purpose | Governance | Approx. count | Primary use |
| ICD-10-cm | Diagnosis coding | CDC/NCHS | ~70,000 | All settings, diagnoses, and reasons for visits |
| ICD-10-pcs | Inpatient procedure coding | CMS | ~87,000 | Hospital inpatient procedures and grouping |
| CPT (level I) | Services and diagnostic services | AMA | ~10,000 | Outpatient services and professional billing |
| HCPCS Level II | Supplies, drugs, DME, prosthetics | CMS | ~7,000 | Items not in CPT: ambulance, equipment, supplies |
| DRG | Payment grouping | CMS | ~700 | Inpatient pricing and hospital reimbursement |
Simplify the medical coding process with Tebra
Navigating ICD-10 and related code sets doesn’t have to be daunting. With the right tools, healthcare providers and billers can improve accuracy, maintain compliance, and minimize denials while protecting margins and patient trust. Strong documentation leads to clean claims, better data, and smoother workflows from charting to follow-up.
Tebra’s EHR software supports everyday coding with integrated lookups, structured orders, and eRx/ePrescribing that connects diagnoses to medications and services. Billing features enable teams to post charges and reconcile payments, while digital communications keep patients informed without requiring additional steps.
For private practices, that means fewer hand-offs and fewer surprises. You focus on care while the system helps streamline routine tasks, keeps information in one place, and aligns coding with payer rules. Schedule a free, personalized demo today and see how Tebra can improve your workflow.

FAQs
Quick answers to common coding questions
You might also be interested in
Optimize your independent practice for growth. Get actionable strategies to create a superior patient experience, retain patients, and support your staff while growing your medical practice sustainably and profitably.
- Current Version – Nov 18, 2025Written by: Jean LeeChanges: This article was updated to include the most relevant and up-to-date information available.





